A day with a social worker: compassion and support for families
Listeners, problem-solvers, advocates, and much more, social workers wear many hats. Mission Hospice social worker Elizabeth (Tess) Rogers says that her job is “pairing what resources and support are available with what families are ready for.”
Tess aims to see each of her patients every two weeks, or more often as needed – patients’ needs may change over time. Some days Tess visits three or four patients; other days she spends more time making calls, faxing paperwork, or following up on MediCal or VA benefits.
“While nurses and physicians help with physical pain, we can help with emotional pain, resources, and counseling – for patients and families,” Tess explains. “Our job is to hold space for everyone to express their feelings, their fears, and their wishes, and to be the mediator as needed.”
On a recent day, Tess started with a phone call from a nurse who needed some advice about how to assist a struggling family. “It’s part of our job to support our fellow team members,” Tess explains. “We have such a supportive, compassionate team – we all have each others’ backs.”
 By the time this conversation has finished, Tess has arrived at the Millbrae home of her first patient.
By the time this conversation has finished, Tess has arrived at the Millbrae home of her first patient.
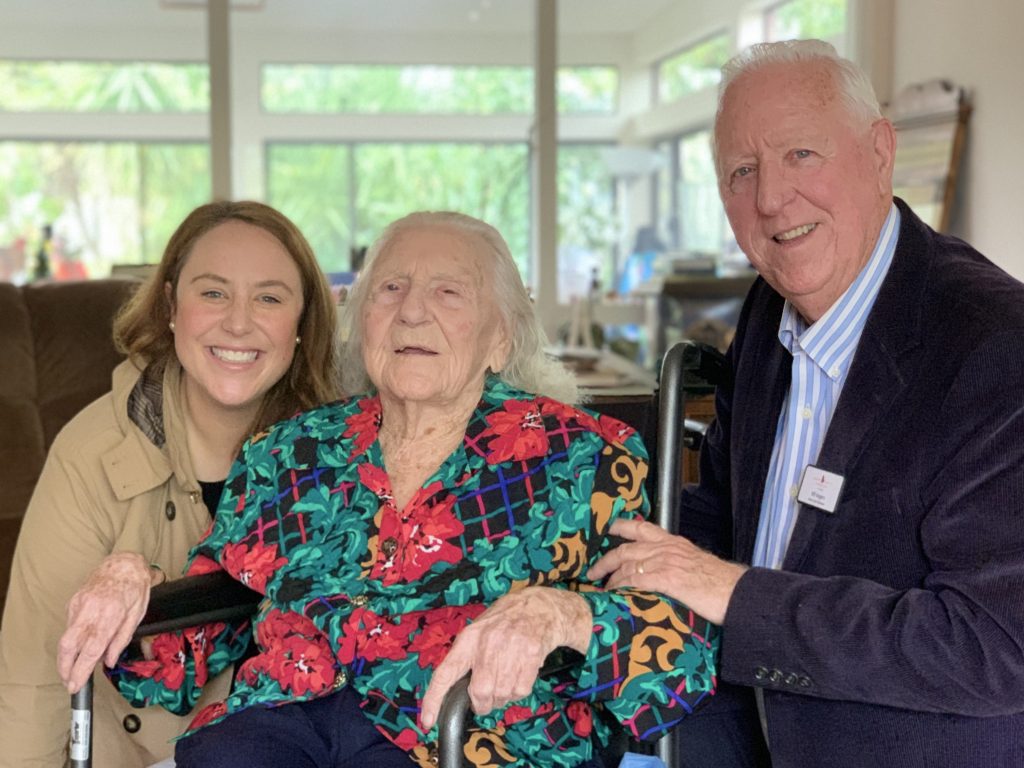
Opal, a retired professor with Alzheimer’s disease, recently turned 102, and Tess brings with her a small box of doughnuts to celebrate. She’s welcomed like family by both Opal and her caregiver.
With her wheelchair scooted up to the dining room table, Opal eats breakfast while Tess visits. Warm and gentle, Tess asks Opal about her childhood on a Mississippi farm, skillfully working in questions about her pain level and mood.
“Is there anything on your heart that you want to talk about?” Tess asks. Opal says she wouldn’t change a thing about her life, something Tess says is a good reminder of staying in the present and expressing gratitude.
Tess also reassures the caregiver that she’s doing a good job. “Part of my role is to encourage the patient and family, to let them know that they can do this,” she says.
While stopping for a second cup of coffee, Tess makes some notes about the visit for other members of the care team. And later, she will – as usual – call Opal’s daughter Pam with an update. She explains: “Sometimes I work more with the family than with the patient. A lot of our work is helping families accept what is happening, while acknowledging their pain, grief, and sadness.”
Tess’ next stop is at the Redwood City home of John and Michelle. When John, who has prostate cancer, started hospice care, his wife was reluctant to accept social work support. After Tess offered to stay with him so Michelle could attend her church meetings, that built trust that allowed Tess to provide even more meaningful support to the family.
Tess explains that much of her work with this family has been counseling. “Both of them were angry about John’s disease. I was able to help them talk through it so that they could project their anger onto the disease, and not each other.” Tess also facilitated family meetings with their two adult daughters, who wanted to be more involved in care and decisionmaking.
Today, Tess talks to John about his veterans’ benefits, which she facilitated so that he could get the VA caregiver he had earned. Helping people navigate benefits and find resources is an important part of the social work role.
Only partly joking, Tess says that social workers are “the forms people.” In addition to helping people navigate insurance benefits, MediCal and Medicare, and paid family leave, they help people complete Advance Health Care Directives and review their POLST forms.
Social workers also help navigate care at a very practical level. “We can start the conversation about where the best place is for care. We help determine whether the patient is safe in the home, or needs care beyond what family members can provide.”
 After her visit with John and Michelle, Tess heads north again to her patient in an assisted living facility in Burlingame. Harold, at 93, has congestive heart failure. In a single week, he moved into the facility and started hospice care – quite a change for the vibrant, independent man. Tess says that she visited weekly at first, to help him adjust to his new environment.
After her visit with John and Michelle, Tess heads north again to her patient in an assisted living facility in Burlingame. Harold, at 93, has congestive heart failure. In a single week, he moved into the facility and started hospice care – quite a change for the vibrant, independent man. Tess says that she visited weekly at first, to help him adjust to his new environment.
When he first moved there, she orchestrated a care conference with Harold and his children, the entire Mission Hospice team, and facility staff. Tess explains that “these meetings lay the foundation for the patient’s care, who does what, and making sure the family understands how we can support them. We are always there to advocate for the patient.”
The staff at Harold’s home now knows Tess well. As part of her visit with Harold, Tess observes and records his appearance, eating habits, and alertness.
Harold is a big sports fan, something he loves to share with his Mission Hospice volunteer – who just happens to be Tess’ dad Bill. The father-daughter duo often visit patients together. “It’s the biggest joy to be able to do this work together,” says Tess. “I think patients get a sense that they’re really being cared for – it’s a family thing.”
Her main objective is to help Harold review his life and prepare to die peacefully. Over the past few months, Tess has talked with him about his childhood and the many things he has accomplished. She’s also helping him through depression and grief from his wife’s death four years earlier. “My job is to hear his story, to witness and help him process his life.”
Back in the Mission Hospice office, Tess will finish her notes for these patients, plan tomorrow’s visits, make a few phone calls, and check in with her colleagues – an important part of her day. “Experiencing someone’s vulnerabilities is such an honor – but it can be difficult. It’s so helpful to be able to unpack that with a colleague who gets it,” she says.
“Ultimately, bearing witness to someone’s anger or grief is the biggest gift. That’s when I feel like I am really helping. That’s what is so rewarding about this work.”
Spiritual care: Helping patients find peace
 by Rachel Rosenberg, Spiritual Counselor
by Rachel Rosenberg, Spiritual Counselor
Many people are surprised to learn the range of services we offer as Spiritual Counselors. Our role on the hospice team is to assess patients’ spiritual and emotional needs and barriers to peace.
What this means is different for each person. Some express their spirituality through religion; others express it through nature, the arts, or in ways that help them find their place in the universe.
When people are facing death, they may find solace in sharing life stories and expressing gratitude and hope. This was the case for our hospice patient Pedro.
When we met, Pedro was sitting on the couch in the modest Redwood City apartment he shared with his wife and two daughters. His arms, muscular from years of construction work, hung idly at his sides. He told me he missed working and being able to provide for his family. We agreed that it can be hard to accept so much help.
Over the course of several months, Pedro and I explored his many concerns, including whether he would return to his native Guatemala to die. When I asked him, “what is most important to you now,” a question that reflected his diminishing time on earth, Pedro did not hesitate. He wanted to have peace in his family, and leave his daughters, ages 16 and 18, with positive memories.
With his goal in mind, Pedro and I set out to draft legacy letters for his daughters. He thought about his relationship with them, and his hopes for a future that he would not live to see.
As he found words to express his love, I recorded his thoughts on paper. His cancer had made it difficult to write and think clearly.
Despite these struggles, Pedro had the determination of a man who knew this would be one of his final acts. We both knew that when he is gone, these letters will remain as a testimony to his life and the love he holds for his family.
He thanked his daughters for being the center of his attention. He wished them the same blessing of enjoyment in this life that he was able to have. He bestowed words of fatherly advice, allowing himself to give them guidance one last time.
After we’d finished the letter, Pedro told me he felt liberated. This process of expressing his final wishes made his heart lighter and more peaceful. In a time governed by pain, fatigue, and loss of control, Pedro’s letter writing gave him the gift of choosing his legacy and the space in which to unburden his heavy heart.
Home health aides are a healing presence for patients and families
Our home health aides (HHAs) often spend more time in patients’ homes than anyone else on the care team. Many times, they become trusted friends and confidants, developing close relationships with patients.
HHAs are caregivers, personal attendants, teachers, companions, and much more. They help patients get in and out of bed, bathe, and wash their hair – even if the patient is bed-bound. They change linens. They can offer light massage and apply lotion, which many people find soothing.
 “Our HHAs teach families how to look after their loved ones – most of them have never done this kind of care before,” says Elle James, HHA Manager and Senior Nurse Educator. “Most importantly, they help patients maintain their dignity and feel cared for.”
“Our HHAs teach families how to look after their loved ones – most of them have never done this kind of care before,” says Elle James, HHA Manager and Senior Nurse Educator. “Most importantly, they help patients maintain their dignity and feel cared for.”
Our agency currently has 25 home health aides, each with years of experience. To a person, they say that one of the things they love about working at Mission Hospice is that they are given the time they need to be fully present.
Ana Juarez says this means “we can give the patient our time and attention. We don’t have to rush. And we are trusted to know what is best for the patient.”
A visit from an HHA can be something to look forward to, especially for patients who are house-bound. As Tommy Joe says, “we can be the highlight of their day.”
His colleague Mitch Park concurs. “I ask them to share their stories, and that’s what they look forward to. They could do without the bath!”
Finding a connection with a patient is a good way to establish rapport and trust. Tommy says that he is often able to connect through sports. “It gives us something to talk about and share,” he says.
Mitch agrees. “Usually when someone has a terminal disease, people treat them differently,” he says. “I walk in and I say, ‘Did you see the game last night?’ It’s like a breath of fresh air for them.”
JoGrace Kotico sometimes connects with people through music. She remembers a patient who had served in the Army, who really liked the national anthem. “He wanted me to sing that to him as I cared for him,” she said, laughing about the difficulty of the tune. “I practiced in the car on the way to his house! And on the day he died, I was holding his hand and singing to him.”
These kinds of connections are one reason Mission Hospice is committed to keeping the same care team around patients who move between programs – say, from Palliative Care to Hospice. At a time when so much is changing in their lives, we can offer patients and families the comfort and stability of trusted relationships.
“We talk a lot about not just the physicality of the home health aide role, but the humanness of it,” says Elle. “They do so much more than just provide care. Our HHAs are a healing presence.”
Michael Teutschel and Dr. Gary Pasternak receive awards for service
February 2017
At last month’s 38th Anniversary Celebration at the Sharon Heights Golf & Country Club in Menlo Park, Mission Hospice honored two people who are very special to our organization and our community.

Special Recognition Award winner Dr. Gary Pasternak (center) and 2017 Lotus Award winner Michael Teutschel (second from R) with (L to R) CEO Dwight Wilson, Chair Dr. Stephen Weller, and past Chair Judy DiPaolo at our 38th Anniversary Celebration.
The Lotus Award, created to recognize individuals who have shown outstanding support of the organization, was presented to Michael Teutschel. Mike has served on our Board of Directors for well over a decade, and just completed a term as co-Treasurer.
Lotus Committee member Sheila Young says that Mike was nominated for the award by a number of people and was the committee’s overwhelming favorite.
For years, says Sheila, “Board Chairs have turned to Mike as the go-to person for advice and input. He has excellent judgment and wisdom, and an invaluable ability to see all issues clearly.”
Sheila says Mike’s board colleagues respect his calm leadership. “He listens respectfully, hearing all sides. When he speaks up, people listen. He is a skilled communicator, a peacemaker, and a clear thinker,” she continues. “His ability to synthesize really helps the board come to an understanding on complex topics. And he does this all with a great sense of humor!”
Mission Hospice also presented Medical Director Dr. Gary Pasternak with the Special Recognition Award.
Committee Chair Mary Chigos, RN, says that Dr. Gary is respected throughout the community for his compassion and patient-centered care. His leadership in hospice and palliative care extended to his vision for the hospice house, which was key to inspiring others to support the project.
“People are sometimes afraid of hospice,” says Mary, “but Dr. Gary shows them that they can gain control over their final months, based on their own wishes. He always starts by asking what the patient wants. Dr. Gary is known for going the extra mile for his patients.”
The Mission Hospice family thanks both Mike and Gary for all that they do for the organization and our patients.
Rounds with a hospice nurse: Compassion in action
 When you’re a hospice nurse, each day is different. The schedule, your patients, and their needs vary; the one constant is compassion.
When you’re a hospice nurse, each day is different. The schedule, your patients, and their needs vary; the one constant is compassion.
Mission Hospice RN Case Manager Naoko Ishikawa sees each of her 12-16 patients at least once a week, and more often if their symptoms call for it. She shares the details of a recent day in which she visited five patients.
Her morning starts with a call from Donald, whose mom, Grace – one of Naoko’s patients – had fainted. Naoko heads straight to Grace’s assisted living facility in San Mateo. Donald meets her there, and they review the events with Grace’s caregivers. “We work as a team,” Naoko says, and the trust between them is obvious.
In her 90s, Grace is in bed, frail but conversant. Naoko squats down to look in her eyes. Grace seems reassured by Naoko’s presence, and reports that she feels fine. Naoko takes Grace’s blood pressure, which is strong. She’s confident that Grace’s fainting spell was caused by constipation. Naoko texts Dr. Salpeter to ask about adjusting Grace’s medication to address the issue, and immediately gets the go-ahead.
Naoko gives the caregiver the new instructions, notes this in the patient’s chart, and checks to see that the supplies she’d ordered last week were delivered. An hour later, after making sure Grace is comfortable, Naoko heads to Redwood City to see her first regularly scheduled patient.
 Sharon is thrilled to see Naoko for the second time this week. Almost 90 years old, her husband Herbert has been in hospice care for nine months, and the family has developed a close relationship with their Mission Hospice team. “I’m always relieved when Naoko comes,” Sharon says.
Sharon is thrilled to see Naoko for the second time this week. Almost 90 years old, her husband Herbert has been in hospice care for nine months, and the family has developed a close relationship with their Mission Hospice team. “I’m always relieved when Naoko comes,” Sharon says.
Herbert is watching TV in the living room, and Naoko scoots a chair up close to him. “What did you eat this morning?” she asks. “How is your stomach feeling?” His voice is quiet; he is wheezing, and hard to understand. “Are you dizzy? No? Are you nauseous?”
Naoko is a calm, gentle presence. She takes his vital signs and listens to his stomach. She can tell he needs a suppository to help relieve his constipation – a common problem at the end of life.
With that taken care of, Naoko checks on his pain. She reminds Sharon how to recognize when he’s in pain, and when it would be appropriate to apply a heating pad or give him medicine.
Being a caregiver can be exhausting. As they chat at the kitchen table, Naoko reminds Sharon that she can call any time for support. Naoko assures her she’ll be back in a few days. The visit has lasted well over an hour.
Back in San Mateo, Naoko’s next patient, Lillian, is in a 12-bed assisted living facility. The nurse meets with her caregivers to review changes in Lillian’s condition, making sure all of their questions are answered. Coordination with facility staff is an essential part of her job.
Almost 101, Lillian is comfortably asleep. Naoko sits quietly next to her, watching her breathe. She feels Lillian’s feet to assess her circulation. Naoko also checks Lillian’s supplies. Pads and gloves are running low, so Naoko texts a resupply order that will be delivered tomorrow.
Back in the car, Naoko says she drives an average of about 100 miles a day visiting patients throughout the peninsula. Her radio is tuned to classical music, which helps relax her between visits.
Her next stop is in Burlingame to see Vern, who recently injured his arm in a fall. She adds gauze and tape to her bag before heading into his board and care facility.
 Naoko is greeted warmly; she’s been working with the staff here for several months. In the office, Naoko pulls out Vern’s binder, which contains his plan of care, chart of medicines, and visit notes. She makes a mental note that one of his medicines needs to be refilled.
Naoko is greeted warmly; she’s been working with the staff here for several months. In the office, Naoko pulls out Vern’s binder, which contains his plan of care, chart of medicines, and visit notes. She makes a mental note that one of his medicines needs to be refilled.
In Vern’s suite, Naoko cleans his wound, letting him know it’s healing well. As she works, she asks about his pain and his sleep. Vern’s neurodegenerative disease makes him hard to understand, but Naoko makes out his words.
She is kind and gentle, laughing with him. “We build trust with patients over time,” she says. “When I spend months caring for patients, I really get to know them and their families.”
She tells Vern that she’ll be back in a few days for his next dressing change. Back in the parking lot, she calls the pharmacy for the refill; Dr. Lee has already approved it, and the medication will be delivered the next day.
Her last visit today is to Rita, who lives with her husband Alan in a retirement community. Naoko especially likes seeing patients in this neighborhood of San Mateo, because the nearby Japanese garden is one of her favorite spots for a break.
First, Naoko confers with the staff at the community, working out how they can all support Rita and Alan – her full-time caregiver.
The couple’s lovely condo is filled with orchids, art, and family photos. When Naoko arrives, Rita is resting in bed; Alan is making sandwiches.
Rita is battling lung cancer and shingles. Oxygen makes it easier for her to breathe, but she’s short of breath, and getting around takes some effort. Naoko listens to Rita’s lungs, and notices some swelling in her ankles. The nurse reminds her to keep her feet elevated – the goal is to keep Rita ambulatory.
Naoko also recommends that Rita use her shower chair, which will help save her energy “for something better.” Rita smiles and nods – she would like to be able to resume visits with her friends.
Alan and Naoko move to the living room, letting Rita rest. Respectful of the fact that independence is important to the couple, she gently reminds Alan that his Mission Hospice social worker can help him find in-home help when he is ready. This kind of teamwork is part of what Naoko loves about Mission Hospice. “I get a lot of support here,” she says.
When she is satisfied that Alan has no more questions, Naoko prepares Rita’s medications for the week. Dr. Boblett has already coordinated with the specialist Rita saw yesterday, and Naoko can see the updated medications list on her iPad. She fills Rita’s weekly pillbox, and reminds Alan to make sure Rita takes her medications so she can stay ahead of the pain.
Rita’s eyes are closed, and Naoko whispers her goodbyes. Back in the Mission Hospice office, she will finish her charting for these patients, check in with her colleagues, and finalize details for tomorrow’s visits.
Naoko loves that she can spend the day caring for others (even while seven months pregnant), and considers the time she spends with patients in their home a gift.
“Hospice nursing can be sad – but if I can reduce someone’s pain and help provide a good death, that is the most beautiful thing I can do.”
It was a beautiful day.
Keeping vigil: Being present in someone’s final hours
There are times in our lives when we don’t want to be alone – for many of us, this includes when we are dying. Our vigil program allows us to accompany patients so they are not alone in the last day or two of life. A vigil might allow family members to get some sleep, enjoy a meal, and take a break. For those who don’t have loved ones by their side, a vigil can provide the kind of comfort that can only be offered by another human being.
 “Our goal is to create a safe, peaceful, supportive environment for our patients,” says Volunteer Coordinator Rani Ferreira, who manages the vigil program.
“Our goal is to create a safe, peaceful, supportive environment for our patients,” says Volunteer Coordinator Rani Ferreira, who manages the vigil program.
Vigilers offer companionship and presence. They might dim the lights, share quiet music, read, or simply sit and hold the patient’s hand. Like all of our care, it’s as individual as our patients.
Some vigils are held overnight to allow family members to get some much-needed rest. For patients with no one by their side, vigils might last for several days, with vigil volunteers tagging in for two-hour shifts, offering around-the-clock support. Vigils are wherever our patients are – anywhere from San Mateo to Half Moon Bay to Millbrae to Palo Alto, in a patient’s home or a care facility.
Coordinating a vigil is no small task. When a need arises, Rani puts the word out via email to more than 50 trained vigilers. Once volunteers respond – and they do, even with short notice and middle-of-the-night timeslots – the vigil begins.
Each vigiler interrupts his or her life to bring comfort to a perfect stranger. Some drive 45 minutes to be with someone in need. One volunteer takes the bus at 11 at night – and home again at 1am. Others volunteer for late-night shifts despite demands of work and their own families.
For a patient whose sister lives across the country and couldn’t be with her, Mission Hospice vigilers sat by, read, and prayed with her. And they helped her reach her sister by phone for their last conversation, bringing them both a sense of peace.
Another team vigiled for a 77-year-old woman whose large, loving family felt anxious and unprepared for her death. “The vigilers really helped the family understand what to expect,” explains Rani. ”And they were so grateful that the vigil volunteers were with their mom, so they could come and go as they needed to.”
In Mission House, vigilers accompanied a man with end-stage Alzheimer’s. After nearly a dozen volunteers had taken their turns, the last vigiler knew that the patient’s wife and son were on their way to the house. When her shift was up, she stayed by his side so that he was not alone, comforting him as he passed away, peacefully, before his family arrived.
This is the kind of care for which Mission Hospice is known, and the community knows what a difference it makes. Elizabeth, an experienced caregiver at Millbrae Board & Care Home, was moved by seeing our vigil teams in action. “I’ve worked with hospice patients for 14 years,” she says. “I’ve never seen anything like the compassion, presence, and love you all have shown.”
Free Bay Area screenings of “Being Mortal” are part of national dialogue
We are pleased to announce that Mission Hospice will be showing “Being Mortal,” a PBS film adapted from the best-selling book by physician Atul Gawande, M.D. Part of a nationwide dialogue about individual goals for end-of-life, the events are free and open to the public, but reservations are required at MissionHospice.eventbrite.com.
Screenings are scheduled for:
Friday, June 17, 7pm at Trinity Church, 330 Ravenswood, Menlo Park
Friday, June 24, 6:30pm at Senior Coastsiders, 925 Main Street, Half Moon Bay
Thursday, August 25, 6:30 pm at Mission Hospice, 1670 South Amphlett Boulevard, #300, San Mateo
After each screening, audience members can participate in a guided conversation on how to take concrete steps to identify and communicate wishes about end-of-life goals and preferences.
 “This film illustrates the importance of talking with family members about their hopes and dreams around end-of-life,” said Lisa Deal, Chief Clinical Officer for Mission Hospice & Home Care. “We hope to inspire people to do this, by talking about what we might like for our lives – up until the very end.”
“This film illustrates the importance of talking with family members about their hopes and dreams around end-of-life,” said Lisa Deal, Chief Clinical Officer for Mission Hospice & Home Care. “We hope to inspire people to do this, by talking about what we might like for our lives – up until the very end.”
“Being Mortal” investigates the practice of caring for the dying and explores the relationships between patients and their doctors. The film sheds light on how a medical system focused on a cure often leaves out the sensitive conversations that need to happen so a patient’s true wishes can be known and honored at the end.
Mission Hospice is holding these events in partnership with Trinity Church and Senior Coastsiders as part of a national program sponsored by the Hospice Foundation of America.
“The work of Dr. Gawande creates a wonderful opportunity to open up an important conversation within our community and within families,” said Rev. Elizabeth Riley of Trinity Church. “As difficult as it is to talk about the end of life, there is also a deep yearning to find ways to talk about it, and “Being Mortal” gives people a great place to start.”
“This film shows how death is part of life’s journey, and full of personal choices,” said Janie Bono-James, Executive Director of the Coastside Adult Day Health Center in Half Moon Bay.
Seventy percent of Americans say they would prefer to die at home, but nearly 70% die in hospitals and institutions. Ninety percent of Americans know they should have conversations about end-of-life care, yet only 30% have done so. These events are designed to prompt these conversations.
Common myths about hospice care
Our Clinical Outreach Team works to explain hospice care to patients, families, and physicians, and assesses whether patients might benefit from admission to our services.
Every day, our Outreach nurses and social workers explain what hospice is (and what it is not). Here, they debunk some of myths they often encounter.
MYTH: Hospice means you’re going to die immediately.
Outreach Team: Hospice care neither hastens death nor prolongs life. Hospice care begins when the patient’s medical goal changes from seeking a cure to managing symptoms and providing comfort. It’s about making sure that your quality of life is enhanced for the time you have left. Hospice is about comfort, compassion, and support for the patient, family, and caregivers.
MYTH: Hospice care is expensive.
Outreach Team: Fortunately, hospice care is covered by Medicare as well as by most private insurance plans. The majority of our patients use the Medicare hospice benefit, which covers virtually all hospice services – so there is little or no out-of-pocket cost. For patients who do not have Medicare or other insurance, Mission Hospice donors allow us to offer our quality care free of charge for those who need it.
MYTH: If I enter hospice, they will take away my medicines.
Outreach Team: Our goal is to be sure that patients use only the medicines they need. When a patient enters hospice care, our physicians review their prescriptions (together with the patient and the primary care doctor), and decide which are still beneficial to meet the current goals of care. Hospice care gives families the opportunity to discuss the purpose of the medications their loved one is taking.
MYTH: Hospice means I will have to go away somewhere.
Outreach Team: We provide hospice care for patients wherever they are: home, board and care homes, nursing homes, hospitals, and long-term care facilities. For those who can no longer stay in their own homes, our social workers help families find a place with the right level of care; our hospice house will be an option for some patients.
In most cases, entering hospice care means patients can remain at home to receive the support they need.
MYTH: If I start hospice, I won’t be able to see my doctor any more.
Outreach Team: This is definitely not the case! A patient needs the consent of a primary care doctor to begin hospice care. Our medical staff works closely with our patients’ primary care physicians (and specialists as appropriate) to develop individualized care plans. It is important to keep these doctors connected because sometimes patients “graduate” from hospice and will need these doctors to know what their course of care has been.
MYTH: Once you’re on hospice care, you can’t get off.
Outreach Team: Hospice is a choice – not an obligation. You can always change your mind. And you can start hospice care again later, assuming you are still eligible. Medicare lets you use the benefit multiple times. It is not unusual for a patient to begin hospice services because they are so ill they simply cannot function well any longer. When hospice care helps control symptoms, sometimes time will heal the body. If a patient’s condition improves, they can be discharged from hospice and resume medical treatment, returning to hospice care later as needed.
MYTH: Hospice is scary.
Outreach Team: The thought of dying is frightening to many people, but our patients find that hospice care makes it much less scary. Hospice offers compassion, comfort, and a network of support to help patients, families and caregivers through this period of transition.
Hospice is a real gift to families and loved ones, who are supported throughout the process. We coach family members in caregiving (and offer respite care), offer emotional and practical support, help families navigate medical benefits, and of course offer grief counseling. The earlier you start, the more planning and control you have over your future.
Rev. Walter E. Johnson, M. Div.
 February 2015
February 2015
For more than three decades, Rev. Walter E. Johnson, M. Div. and his wife Esther have supported Mission Hospice just about every way possible. They have been Leadership Circle donors for many years. Esther, a Mission Hospice Auxiliary volunteer since 2000, is now a sustaining member. And Walt has ministered to many, many patients and families, including conducting burials at sea. A private pilot, he has performed nearly 1,000 such ceremonies.
In honor of his lifetime commitment, Walt received the Mission Hospice Lotus Award at our 36th anniversary celebration in January. The award was created in 2005 to recognize individuals who have shown outstanding support of Mission Hospice. Kate Breaux, Lotus Award committee chair, said that the committee is grateful for Walt’s many contributions to Mission Hospice. “Walt’s positive nature, calming presence, and supportive thoughts have been a gift to so many patients – as well as staff.”
As chaplain at Peninsula Hospital for 30 years (and at Sequoia Hospital before that), Walt was an early supporter of the hospice movement. “I’ve had a growing commitment to helping people die well,” he said, “and to die with a sense of personal dignity and connection to their families.”
When he retired from the hospital in 1995, it seemed natural that he would become a chaplain for Mission Hospice, where he served for 12 years. And he’s not done yet. “I’m addicted to ministry,” he says, laughing. “I feel so fortunate to be a minister because I can continue practicing even though I’m not formally hired somewhere.”
Witty and warm, Walt is a good listener, and loves to tell a story – especially one with a laugh. “Many people assume that dying is dark and dreary,” he says, “but there’s an amazing number of times when there is laughter and light. Two things indicate that a person is dying well – one, that they can laugh, not take themselves so seriously, and two, that they have a sense of gratitude.”
And he feels thankful for his life’s work. “I have profound appreciation of the patients and the families who allow us to be with them at such a personal and meaningful time in their lives,” he said. “To me, it is an honor to be in people’s homes at these poignant moments.”
The many of us in the Mission Hospice family who have been touched by Walt’s warmth and ministry feel that gratitude as well, and congratulate Walt on his well-earned honor.
My journey with hospice
George Fulvio, Mission Hospice direct care volunteer
 For a few hours each week, I offer emotional support and companionship to patients who are in the final days of their lives. This work has been – along with the birth of my daughter – one of the most spiritual experiences of my life.
For a few hours each week, I offer emotional support and companionship to patients who are in the final days of their lives. This work has been – along with the birth of my daughter – one of the most spiritual experiences of my life.
When I retired from my law practice in 2003, I knew I wanted to be of more service in some way, but hospice was not even on my mind. At a social function, I ran into a former client who was on the Mission Hospice board and suggested that I would be a good hospice volunteer.
This was not what I wanted to do, but I couldn’t stop thinking about it. I hesitated, but with my wife’s encouragement agreed to at least start the training classes.
That was almost ten years ago.
When I knocked on my first patient’s door, my heart was beating double-time as I wondered what was waiting for me. But I have never felt more welcomed into homes than I am as a Mission Hospice volunteer.
Most people I speak with about hospice say that they don’t think they could handle being with people who are dying. I consider it a great honor to be invited into someone’s home when life is so real, when the present is all that matters. In fact, I always ask to be placed with those who are the closest to death because it is with them that I feel my deepest emotions.
Our motto at Mission Hospice is “It’s about life,” which means to me that although our patients are dying, we can help them live their last days.
People often ask me what I talk about with my patients. My answer is always the same: They set the agenda. My place is to listen and be present with them. Sometimes I may read to them, sometimes feed them, and always I listen to them.
In the end, what I do with them is not nearly as meaningful as the simple fact that I am there. I have so many wonderful memories of my relationships with patients.
As each life nears its end, all that is left for me to do is sit quietly with them. They know I am there, and may show it in a smile or a squeeze of my hand.
Then it is over, and I turn them over to God with a prayer. My work is done with these beautiful souls.